That throbbing in your temples, the pressure behind your eyes—is it “just a headache,” or something more? For the millions who experience head pain, mislabeling the problem can lead to ineffective treatments and unnecessary suffering. Understanding the key differences between a common headache and a migraine is the first and most crucial step toward finding true relief.
This guide will help you decode your symptoms, explore targeted management strategies, and know when it’s time to see a doctor.
Table of Contents
Headache vs. Migraine: It’s More Than Just Intensity
While all migraines are a type of headache, not all headaches are migraines. They are distinct conditions with different underlying mechanisms.
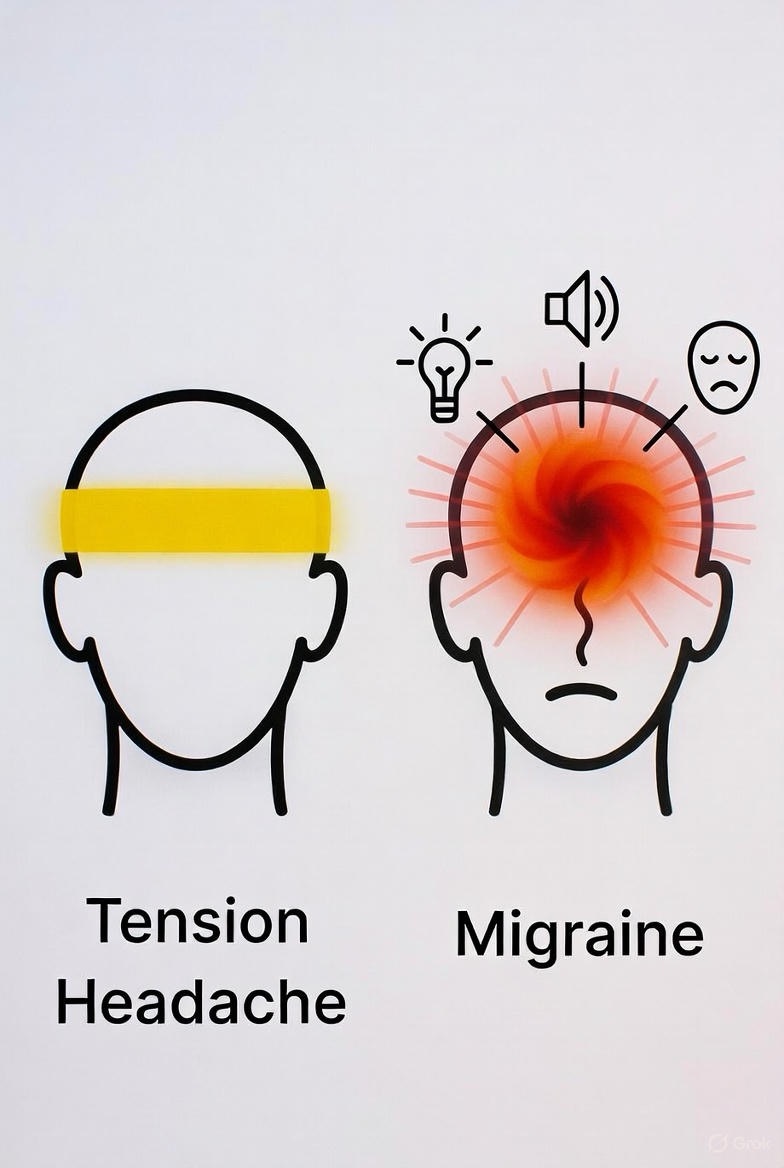
Common Headaches (Tension-Type Headaches):
Think of these as the most frequent visitors. They are typically a response to stress, muscle tension, poor posture, or dehydration.
· Primary Symptom: A constant, dull, aching sensation or feeling of a tight band around the forehead or at the back of the head and neck.
· Pain Level: Usually mild to moderate. It may be annoying, but it rarely stops you from functioning.
· Other Symptoms: Typically, there is no nausea, vomiting, or sensitivity to light/sound. Physical activity usually doesn’t make it worse.
· Duration: Can last from 30 minutes to several hours or even days.
Migraine Attacks: A Neurological Event
Migraine is a complex neurological disorder. It’s not just a bad headache; it’s a cascade of events in the brain that involves nerves, blood vessels, and neurotransmitters.
· Primary Symptom: Intense, throbbing, or pulsing pain, often on one side of the head (but can be both).
· Pain Level: Moderate to severe. It is often debilitating, forcing you to stop activities and seek a dark, quiet room.
· Key Differentiators (The “Migraine Suite”):
· Nausea/Vomiting: A hallmark symptom.
· Sensitivity: Pronounced sensitivity to light (photophobia), sound (phonophobia), and sometimes smells.
· Aura: About 25% of migraineurs experience “aura” before the headache hits. This can include visual disturbances (flashing lights, zigzag lines, blind spots), tingling in the face or hands, or even speech difficulty.
· Aggravation by Activity: Routine physical activity like walking up stairs typically worsens the pain.
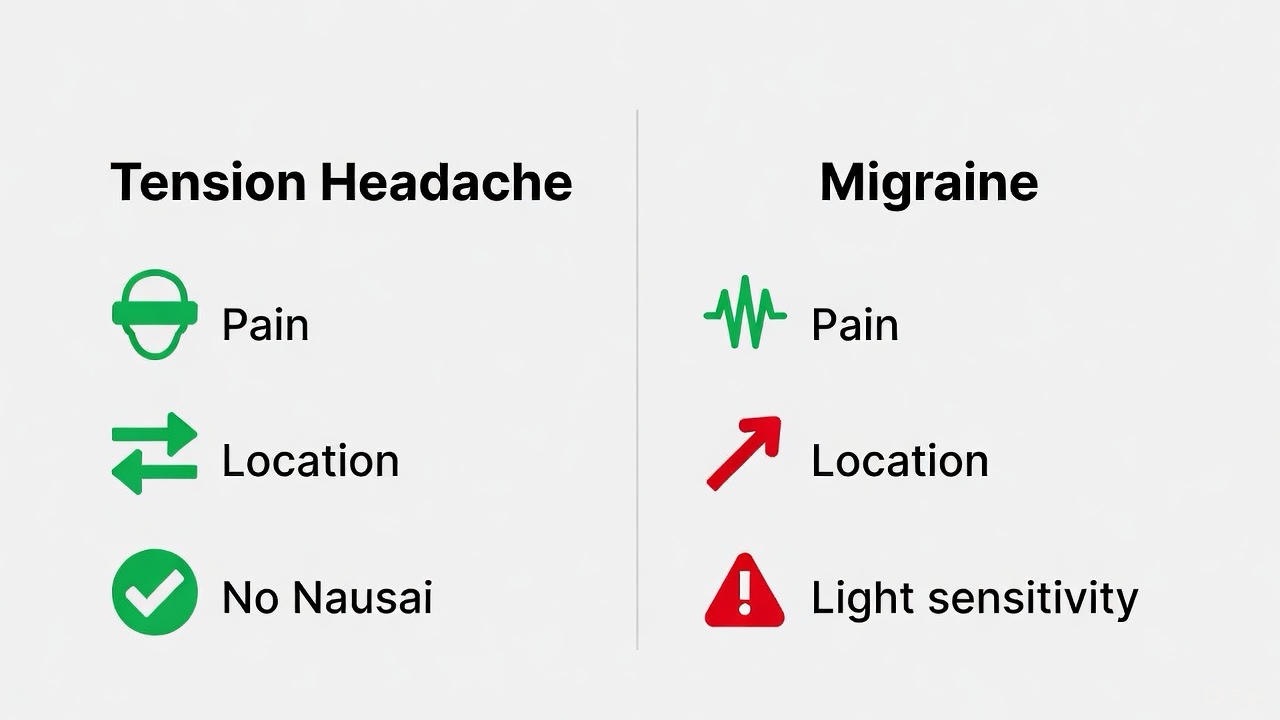
Simple Checklist: Which Sounds Like You?
Symptom
Tension Headache
Migraine
Pain Quality
Dull, tight pressure
Throbbing, pulsating
Pain Location
Both sides, band-like
Often one-sided
Nausea/Vomiting
Rare
Common
Light/Sound Sensitivity
Rare
Very Common
Worsened by Activity
No
Yes
Aura
No
Possible (visual, sensory)
Finding Relief: Tailored Management Strategies
Because their causes differ, so do their most effective treatments.
Managing Tension-Type Headaches:
1. Over-the-Counter (OTC) Relief: Medications like ibuprofen (Advil, Motrin), naproxen (Aleve), or acetaminophen (Tylenol) can be effective when used occasionally.
2. Address the Source: This is key for prevention.
· Stress Management: Practice deep breathing, meditation, or gentle yoga.
· Posture & Ergonomics: Set up a workstation that supports your spine. Take frequent screen breaks.
· Hydration & Regular Meals: Dehydration and low blood sugar are common triggers.
· Physical Therapy/Stretching: For headaches rooted in neck and shoulder tension.
3. Heat Therapy: A warm compress on the neck or shoulders can relax tight muscles.
Managing Migraine Attacks:
Migraine treatment has two pillars: acute (stopping an attack in progress) and preventive (reducing frequency and severity).
Acute/Rescue Treatments:
· OTC Migraine Formulas: Drugs combining acetaminophen, aspirin, and caffeine (like Excedrin Migraine) can help mild-to-moderate attacks.
· Prescription Triptans: These are migraine-specific drugs (like sumatriptan/Imitrex) that constrict blood vessels and block pain pathways in the brain. They are most effective when taken at the first sign of an attack.
· CGRP Receptor Antagonists (Gepants): A newer class of drugs (like ubrogepant/Ubrelvy) that block a protein involved in migraine pain, often with fewer side effects than triptans.
· The “Dark Room” Protocol: At the first hint of migraine, retreat to a quiet, dark room. Apply an ice pack to your forehead or neck. This simple step can sometimes halt a mild attack in its tracks.
Preventive Strategies (If you have frequent attacks):
· Prescription Preventatives: These are taken daily and can include certain blood pressure medications, antidepressants, anti-seizure drugs, or the newer CGRP monoclonal antibody injections (like Aimovig, Emgality).
· Identify and Avoid Triggers: Keep a detailed headache diary. Common triggers include specific foods (aged cheese, processed meats), hormonal changes, sleep disruption, strong smells, and weather changes.
· Lifestyle Foundation: Regular sleep, consistent meals, and aerobic exercise are powerful, non-drug preventive tools for migraine.
· Neuromodulation Devices: FDA-cleared devices like Cefaly or gammaCore use electrical or magnetic pulses to prevent and treat migraines.
When to See a Doctor
Consult a healthcare professional—a primary care doctor or a neurologist—if:
· Your headache pattern changes or becomes more severe.
· You experience what you think is your first migraine.
· OTC medications are no longer effective.
· You have headaches more than 15 days a month.
· You experience a “thunderclap” headache (sudden, severe peak in seconds).
· Your headache is accompanied by fever, stiff neck, confusion, seizure, or double vision.
The Bottom Line: Listening to your body’s specific signals is everything. A tension headache asks for relaxation and simple care. A migraine demands recognition as a neurological event requiring targeted strategies. By accurately identifying your experience, you can move past guesswork and partner with your doctor to build a personalized plan for lasting relief.
FAQs
1. Q: Can a tension headache turn into a migraine?
A: While they are distinct conditions, it’s possible for a severe tension-type headache to trigger a migraine episode in someone prone to them, especially if the pain and stress create a cascade of neurological changes. However, a typical tension headache does not “transform” into the same biological event as a migraine.
2. Q: I have pressure but no throbbing. Could it still be a migraine?
A: Yes. While throbbing is classic, migraine pain can sometimes be described as a “pressure” or “drilling” sensation. The key differentiators are the associated symptoms: if your pressure headache is accompanied by nausea, light sensitivity, or is worsened by activity, it may still be a migraine variant.
3. Q: What does a migraine “aura” actually look/feel like?
A: Aura symptoms are reversible and typically last 20-60 minutes before the headache. They are neurological and can include:
· Sensory: A “pins and needles” sensation that starts in one hand and travels up the arm to the face (known as “cheiro-oral paresthesia”).
· Speech/Language: Temporary difficulty finding words or speaking clearly.
4. Q: Is it a sinus headache or a migraine?
A: True sinus headaches are rare and are caused by active infection (sinusitis) with thick, colored discharge, fever, and pain over the cheekbones/forehead that worsens with bending forward. Many self-diagnosed “sinus headaches” are actually migraines. Migraine pain can concentrate around the sinus areas, causing confusion. If you lack cold/flu symptoms and your “sinus” headaches have light sensitivity/nausea, suspect migraine.
5. Q: Excedrin Migraine helps me. Does that confirm I have migraines?
A: Not definitively. Excedrin Migraine (acetaminophen + aspirin + caffeine) can be effective for both severe tension headaches and mild-to-moderate migraines. Its success suggests you might have migraines, especially if OTC ibuprofen alone fails, but a diagnosis should be based on your full symptom profile.
6. Q: I’m afraid of prescription medication side effects. What are my natural options?
A: Several evidence-based natural strategies can be effective, especially for prevention:
· Supplementation: Riboflavin (Vitamin B2 – 400mg/day), Magnesium Glycinate or Citrate (400-500mg/day), and Coenzyme Q10 have clinical support for reducing migraine frequency.
· Behavioral Therapies: Cognitive Behavioral Therapy (CBT) and biofeedback teach you to manage stress responses and body signals that trigger migraines.
· Acupuncture: Shown in studies to be a valuable preventive option for some.
7. Q: Why do I get a headache when I stop drinking coffee?
A: This is a caffeine withdrawal headache, a type of tension headache. Caffeine causes blood vessels to constrict. When you regularly consume it and then stop, the blood vessels dilate, leading to pain. To avoid this, taper your caffeine intake slowly over a week rather than quitting abruptly.
8. Q: What is a “medication overuse headache” and how do I avoid it?
A: Also known as a rebound headache, this occurs when using acute headache medication (even OTC) too frequently (e.g., >10-15 days a month for most drugs) paradoxically causes more frequent, daily headaches. The treatment is to work with a doctor to carefully withdraw from the overused medication and start a preventive regimen.
9. Q: What are the most common migraine triggers?
A: Triggers are highly individual, but common ones include:
· Behavioral: Lack of or too much sleep, stress or the “let-down” after stress, poor posture.
10. Q: Can screen time cause migraines?
A: Absolutely. This is often due to digital eye strain, which can trigger tension headaches. For migraineurs, the blue light, flicker, and glare from screens can be a direct neurological trigger. Use the 20-20-20 rule (look 20 feet away for 20 seconds every 20 minutes), enable night mode filters, and ensure proper screen brightness/contrast.
11. Q: When is a headache a medical emergency?
Use the acronym S.N.O.O.P.
A: Seek immediate medical attention if your headache has any of these red flags:
· S – Sudden, severe (thunderclap) onset.
· N – Neurological symptoms like confusion, weakness, numbness, vision loss, or difficulty speaking.
· O – Onset after age 50 (new, persistent headache).
· O – Other systemic signs like high fever, stiff neck, or rash.
· P – Pattern change (a dramatic change in your usual headache).
12. Q: My headaches are worse in the morning. Is this serious?
A: Morning headaches can have benign causes like sleep apnea, teeth grinding (bruxism), or poor sleep posture. However, a new pattern of headaches that wake you up or are worst in the morning should be evaluated by a doctor to rule out other causes like sleep disorders or, more rarely, increased intracranial pressure.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.